Free Helpline
We are here to assist you.
Health Advisor
+91-8877772277Available 7 days a week
10:00 AM – 6:00 PM to support you with urgent concerns and guide you toward the right care.
We are here to assist you.
Health Advisor
+91-8877772277Available 7 days a week
10:00 AM – 6:00 PM to support you with urgent concerns and guide you toward the right care.
Stevens-Johnson Syndrome (SJS) is a rare but severe medical emergency causing blistering and detachment of the skin and mucous membranes. Learn about its causes, symptoms, diagnosis, treatment, and prevention.

Stevens-Johnson Syndrome (SJS) is a rare but severe medical emergency that affects the skin and mucous membranes. It is characterized by a blistering rash that can cause the skin to detach. SJS is closely related to Toxic Epidermal Necrolysis (TEN), with TEN being a more severe form of the same condition. In SJS, the affected skin area is typically less than 10% of the body's total surface area, while in TEN, it is more than 30%. The overlap between these two conditions is known as SJS/TEN, affecting 10-30% of the body's surface.
The condition was once known as Lyell’s syndrome and is sometimes mistakenly referred to as “Steven Johnson syndrome.” It is crucial to understand that SJS is a life-threatening condition that requires immediate medical attention. If you suspect you or someone you know might have SJS, it is vital to call emergency services or go to the nearest emergency care facility without delay.
The hallmark symptom of SJS is a blistering rash that primarily affects the mucous membranes. The onset of symptoms can be preceded by flu-like symptoms for 1 to 3 days before the rash appears. These early symptoms often include:
When the rash begins, it may appear as pink spots with darker centers. These spots can be flat or slightly raised and may progress to a darker red or purple color. The rash typically starts on the face and chest and then spreads to the mucous membranes, most commonly affecting the lips and the inside of the mouth. However, it can also appear on:
In some areas, the rash can blister, leading to the death and peeling of the epidermis, the outermost layer of the skin. Pictures of SJS rashes often show widespread blistering and redness, affecting both the skin and mucous membranes. The rash can occur anywhere on the body, but it usually begins on the face or chest and then spreads. Approximately half of individuals with SJS develop rashes on three or more separate mucosal sites.
SJS is most commonly triggered by an adverse immune response to certain medications. In some instances, infections can also lead to SJS. Experts suggest that a combination of medications and infections might contribute to the development of SJS in some cases, while in others, the exact trigger remains unidentified.
While over 100 medications have been associated with SJS, they generally fall into a few main categories. SJS typically develops within a few days to 8 weeks after starting a new medication.
Two main categories of infections are associated with SJS:
While rare, there have been reports of SJS linked to vaccinations. However, there is no clear pattern or specific vaccine consistently associated with the condition.
Certain factors can increase an individual's risk of developing SJS:
Diagnosing SJS involves a thorough medical history, physical examination, and specific tests. Doctors will look for the characteristic rash involving the skin and mucous membranes. Key diagnostic steps include:
SJS is a medical emergency requiring immediate hospitalization, often in an intensive care unit (ICU) or a specialized burn unit. The primary goals of treatment are to stop the progression of the condition, manage symptoms, and prevent complications.
Recovery from SJS can be lengthy, and long-term complications can occur, including skin scarring, vision problems, and chronic pain.
While SJS cannot always be prevented, certain measures can help reduce the risk:
It is imperative to seek immediate medical attention if you experience any of the following symptoms, especially if you have recently started a new medication:
If you suspect Stevens-Johnson Syndrome, do not wait. Call emergency services or go to the nearest emergency room immediately. Early diagnosis and treatment are critical for a better outcome.
No, Stevens-Johnson Syndrome itself is not contagious. It is an immune system reaction to a medication or infection, not an infectious disease that can be passed from person to person.
Recovery time varies greatly depending on the severity of the SJS and the individual's overall health. It can take weeks to months for the skin to heal, and some long-term complications may persist.
Yes, it is possible for SJS to occur more than once, especially if the individual is exposed to the same trigger medication or a cross-reactive medication. It is crucial to avoid any known triggers in the future.
SJS and TEN are on a spectrum of the same severe skin reaction. The main difference lies in the extent of skin detachment. SJS affects less than 10% of the body's surface area, SJS/TEN affects 10-30%, and TEN affects more than 30%.
Yes, long-term effects can include chronic dry eye, vision impairment, skin scarring, changes in skin pigmentation, chronic pain, and sometimes respiratory issues.
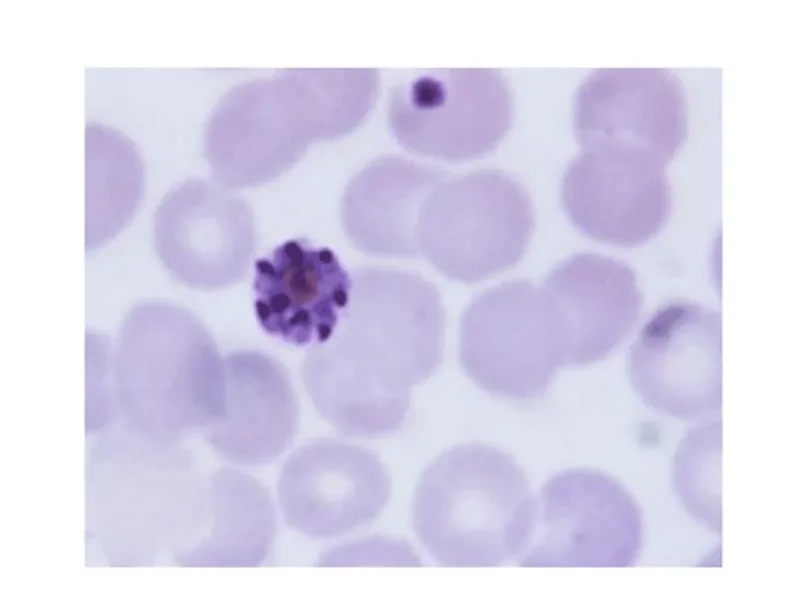
Understand the peripheral blood smear test for malaria diagnosis, its procedure, and what results mean for patients.
April 20, 2026
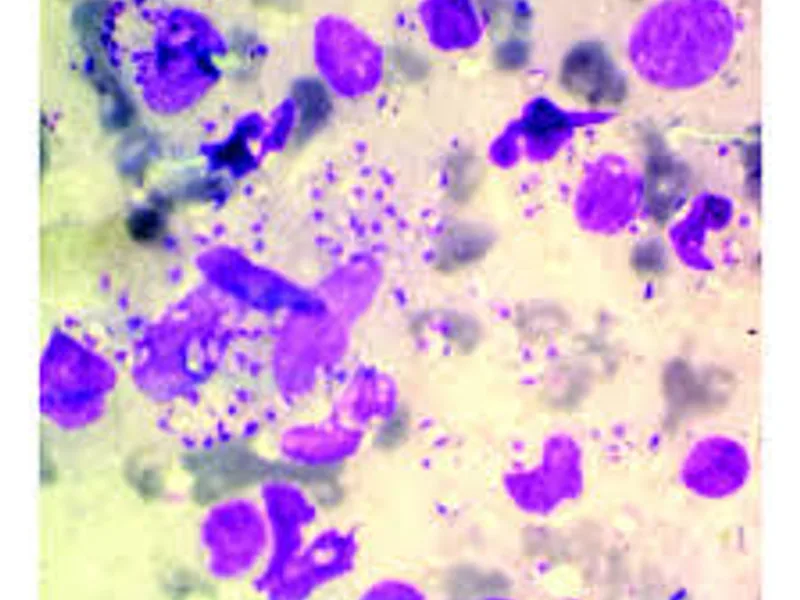
Discover how specialized staining techniques, like Giemsa, are crucial for accurately diagnosing Leishmaniasis, identifying the parasite, and guiding timely treatment. Understand this key diagnostic approach.
April 20, 2026
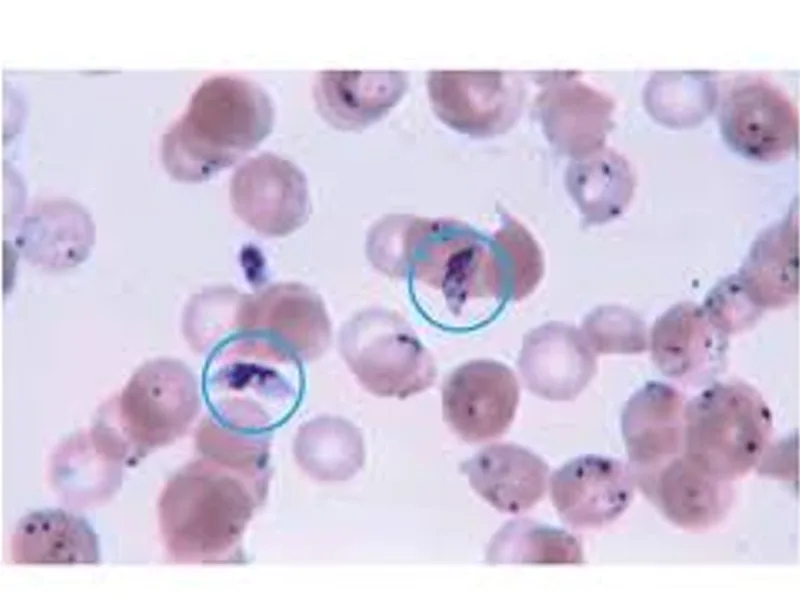
Understand the peripheral blood smear test for malaria diagnosis, its procedure, and why it's a vital tool in combating this disease.
April 20, 2026