Free Helpline
We are here to assist you.
Health Advisor
+91-8877772277Available 7 days a week
10:00 AM – 6:00 PM to support you with urgent concerns and guide you toward the right care.
We are here to assist you.
Health Advisor
+91-8877772277Available 7 days a week
10:00 AM – 6:00 PM to support you with urgent concerns and guide you toward the right care.
Explore the connection between Ulcerative Colitis and Pyoderma Gangrenosum, a rare skin condition. Learn about symptoms, causes, diagnosis, and treatment options.

Understanding Pyoderma Gangrenosum in the Context of Ulcerative Colitis Ulcerative Colitis (UC) is a chronic inflammatory bowel disease (IBD) that primarily affects the large intestine. While its main impact is on the digestive system, UC can also lead to a range of symptoms and complications that affect other parts of the body, known as extra-intestinal manifestations. One such rare but serious condition is Pyoderma Gangrenosum (PG). This article aims to shed light on the connection between UC and PG, helping individuals in India understand the risks, symptoms, diagnosis, and management of this skin condition. What is Pyoderma Gangrenosum? Pyoderma Gangrenosum is a rare, non-infectious inflammatory skin disorder characterized by the rapid development of painful sores or ulcers. These ulcers typically start as small, red or purplish bumps that can quickly enlarge and deepen, often with a distinctive blue or violet border. While the exact cause of PG is not fully understood, it is believed to be an autoimmune condition, where the body's immune system mistakenly attacks healthy tissues, leading to inflammation and tissue damage. The Link Between Ulcerative Colitis and Pyoderma Gangrenosum Research indicates that individuals with inflammatory bowel diseases, including Ulcerative Colitis and Crohn's disease, have a higher likelihood of developing extra-intestinal manifestations. While Crohn's disease patients tend to experience these manifestations more frequently, UC patients are also at an increased risk for conditions like Pyoderma Gangrenosum. It's estimated that about 2% of people with Ulcerative Colitis may develop PG. Furthermore, approximately 50% of individuals diagnosed with Pyoderma Gangrenosum have an underlying related disorder, such as UC, rheumatoid arthritis, or Crohn's disease. The skin manifestations of UC often appear within the first two years of the initial diagnosis. Is Pyoderma Gangrenosum an Autoimmune Disorder? While not definitively proven, the prevailing theory among medical professionals is that Pyoderma Gangrenosum is indeed an autoimmune disorder. This is supported by its higher prevalence in individuals with other autoimmune conditions like Ulcerative Colitis. The exact mechanism linking UC and PG is still under investigation, but the autoimmune hypothesis suggests that an overactive immune response in UC might trigger a similar response in the skin, leading to PG. Symptoms of Pyoderma Gangrenosum The appearance and progression of Pyoderma Gangrenosum can vary, and doctors sometimes classify lesions based on their presentation. The common symptoms include: Initial Presentation: Small, red or purplish bumps that may develop into blisters. Ulcer Formation: These blisters can rupture, forming open sores that are often very painful. The edges of these ulcers are typically deep blue or violet. Progression: The sores can spread rapidly, becoming wider and deeper over time. Doctors may categorize PG into four main types: Atypical/Bullous: Characterized by superficial blisters, often on the hands. This type can sometimes be associated with underlying cancers like leukemia. Classic: Typically begins on the legs, causing deep ulcerations. These lesions can also appear on the head, neck, trunk, and near surgical openings (like a stoma). Pustular: This type is more common in individuals with IBD like UC. It presents as painful, pus-filled bumps, usually on the arms and legs. Vegetative: Lesions that are not typically painful but persist for a long time. It's important to note that PG can sometimes be misdiagnosed as other skin conditions, such as infections or vasculitis, due to its varied presentation. Causes and Risk Factors The precise cause of Pyoderma Gangrenosum remains elusive. However, several factors are known to increase the risk: Inflammatory Bowel Diseases: Ulcerative Colitis and Crohn's disease are significant risk factors. Autoimmune Disorders: Conditions like rheumatoid arthritis, lupus, and Sjögren's syndrome. Trauma or Injury: PG can sometimes develop at the site of skin injury, surgery, or even insect bites. Certain Cancers: Though rare, some blood cancers like leukemia have been linked to PG. For individuals with Ulcerative Colitis, the presence of PG indicates that the disease's inflammatory effects extend beyond the gastrointestinal tract. Diagnosis of Pyoderma Gangrenosum Diagnosing Pyoderma Gangrenosum can be challenging due to its similarity to other skin conditions. There is no single definitive test. Diagnosis is typically made based on: Clinical Presentation: A thorough examination of the skin lesions and their characteristic appearance. Medical History: Assessing the patient's history of IBD, autoimmune diseases, or recent injuries. Exclusion of Other Conditions: Doctors will rule out infections (bacterial, fungal, viral), vasculitis, certain cancers, and other skin disorders through tests like skin biopsies, cultures, and blood work. A skin biopsy, while not diagnostic on its own, can help exclude other conditions and may show characteristic inflammatory patterns. Response to Treatment: Sometimes, a diagnosis is confirmed if the lesions show improvement with treatments specifically for PG, such as immunosuppressants. It is crucial for patients with UC experiencing new or worsening skin lesions to consult their doctor promptly for an accurate diagnosis. Treatment for Pyoderma Gangrenosum The primary goal of treating Pyoderma Gangrenosum is to reduce inflammation, manage pain, promote healing, and prevent new lesions from forming. Treatment strategies often involve a multi-faceted approach: Wound Care: Gentle cleansing and appropriate dressings are essential to protect the ulcer and promote healing. Avoid harsh scrubbing. Topical Treatments: Corticosteroid creams or ointments may be applied directly to the lesions. Systemic Medications: These are crucial for controlling the underlying inflammation. Common medications include: Corticosteroids: Oral prednisone is often the first line of treatment to quickly reduce inflammation. Immunosuppressants: Drugs like cyclosporine, tacrolimus, azathioprine, and mycophenolate mofetil are frequently used to suppress the immune system and prevent further damage. Biologics: In some cases, biologic drugs used to treat IBD, such as infliximab or adalimumab, may also be effective for PG. Other Medications: Dapsone, minocycline, and IV immunoglobulin (IVIG) may also be considered. Pain Management: Adequate pain relief is vital, often involving prescription pain medications. Addressing Underlying Conditions: Effective management of Ulcerative Colitis is critical, as controlling the IBD can help in managing PG. Treatment is often tailored to the individual patient, considering the severity of PG, the extent of UC, and the presence of other health conditions. Prevention Strategies Preventing Pyoderma Gangrenosum entirely is difficult, especially given its autoimmune nature and association with IBD. However, some measures can help reduce the risk or severity: Optimal Management of Ulcerative Colitis: Adhering to your prescribed treatment plan for UC is paramount. Keeping the inflammation of UC under control may reduce the likelihood of extra-intestinal manifestations like PG. Careful Wound Management: If you have UC and experience any skin injury, even minor ones, clean and dress the wound carefully to prevent potential triggers for PG. Avoid unnecessary trauma to the skin. Awareness: Being aware of the symptoms of PG and seeking prompt medical attention if they appear is crucial for early diagnosis and treatment, which can prevent severe complications. When to Consult a Doctor If you have Ulcerative Colitis and notice any of the following, it is essential to consult your doctor or gastroenterologist immediately: Sudden appearance of small, red bumps on your skin that rapidly develop into painful sores. Skin lesions with a purplish or blue border. Any new, unexplained, and rapidly worsening skin ulcers, especially if they are painful. Worsening of existing skin lesions. Early intervention is key to managing Pyoderma Gangrenosum effectively and preventing significant scarring or complications. Your doctor will guide you on the appropriate diagnostic steps and treatment plan. Frequently Asked Questions (FAQ) Q1: Can Pyoderma Gangrenosum spread from person to person? No, Pyoderma Gangrenosum is not contagious. It is an inflammatory condition of the skin, not an infection, and therefore cannot be transmitted from one person to another. Q2: How long does it take for Pyoderma Gangrenosum sores to heal? The healing time for Pyoderma Gangrenosum can vary significantly depending on the size and depth of the ulcer, the underlying cause, and the effectiveness of treatment. Healing can take weeks, months, or even longer. Proper wound care and consistent medical treatment are crucial for promoting healing and minimizing scarring. Q3: Is Pyoderma Gangrenosum always painful? While most forms of Pyoderma Gangrenosum are associated with significant pain, the vegetative type is often described as less painful. However, the severity of pain can differ among individuals and lesion types. Q4: Can Pyoderma Gangrenosum occur without Ulcerative Colitis? Yes, Pyoderma Gangrenosum can occur in individuals without any known underlying condition, although it is more common in those with IBD, autoimmune diseases, or certain cancers. When it occurs without an identifiable cause, it is referred to as idiopathic Pyoderma Gangrenosum. Q5: What is the long-term outlook for someone with Ulcerative Colitis and Pyoderma Gangrenosum? The long-term outlook depends on the severity of both conditions and how well they are managed. With appropriate treatment for both UC and PG, many individuals can achieve remission and lead fulfilling lives. However, PG can lead to significant scarring, and recurrent episodes are possible. Close collaboration with your healthcare team is essential for ongoing management and monitoring. This information is intended for general knowledge and informational purposes only, and does not constitute medical advice. It is essential to consult with a qualified healthcare professional for any health concerns or before making any decisions related to your health
In summary, timely diagnosis, evidence-based treatment, and prevention-focused care improve long-term health outcomes.
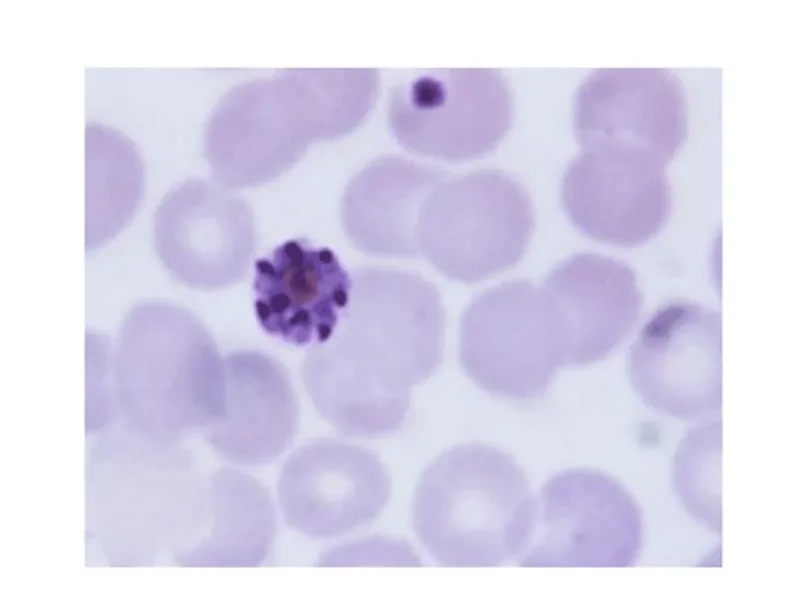
Understand the peripheral blood smear test for malaria diagnosis, its procedure, and what results mean for patients.
April 20, 2026
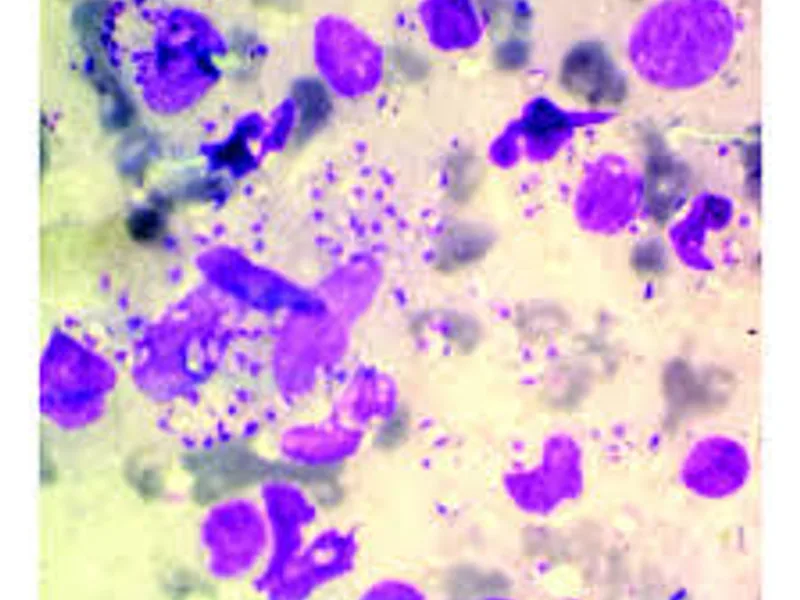
Discover how specialized staining techniques, like Giemsa, are crucial for accurately diagnosing Leishmaniasis, identifying the parasite, and guiding timely treatment. Understand this key diagnostic approach.
April 20, 2026
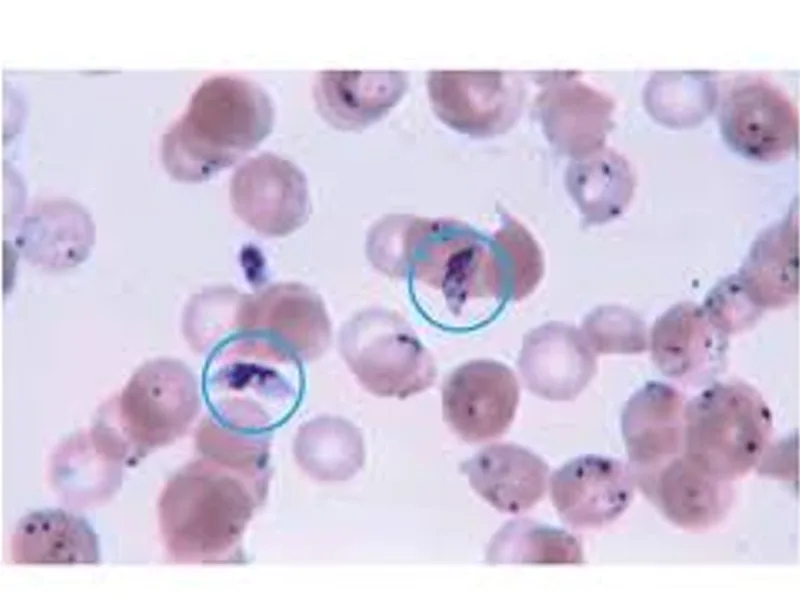
Understand the peripheral blood smear test for malaria diagnosis, its procedure, and why it's a vital tool in combating this disease.
April 20, 2026